
Learn more about our course on Mast Cell Tumour Removal in dogs
Peri-anal mast cell tumour removal
Dr Charles Kuntz is a veterinary surgeon at Southpaws Specialty Surgery for Animals. At Southpaws, Charles performs many different types of surgeries on animals and in this article, he’s going to explain how to remove a grade II peri-anal mast cell tumour.
What is a mast cell tumour?
A mast cell tumour (MCT) is a type of tumour consisting of mast cells. These are a type of white blood cell that is found in different tissues in the body. Mast cell tumours can appear on any part of the body and can look like a lump or bump on the skin; however, they can vary in appearance.
What is a grade II mast cell tumour?
Grade II is the intermediate grade. They can spread to lymph nodes but rarely spread throughout the body. Most grade II MCTs are curable if they are operated on and removed, but more aggressive grade II tumours may require additional treatment.
How do you remove a grade II mast cell tumour?
In the images you’ll see below, Dr Kuntz is removing a peri-anal mass cell tumour.
Here you see the colour volume rendered CT scan showing the MTC on the left-hand side of the rectum.

First electrocautery is used to mark out the proposed surgical incision, which is 2 cm away from the visible MCT. You may notice a bit of anal sphincter contraction, but this is a reflex not that the patient is awake.
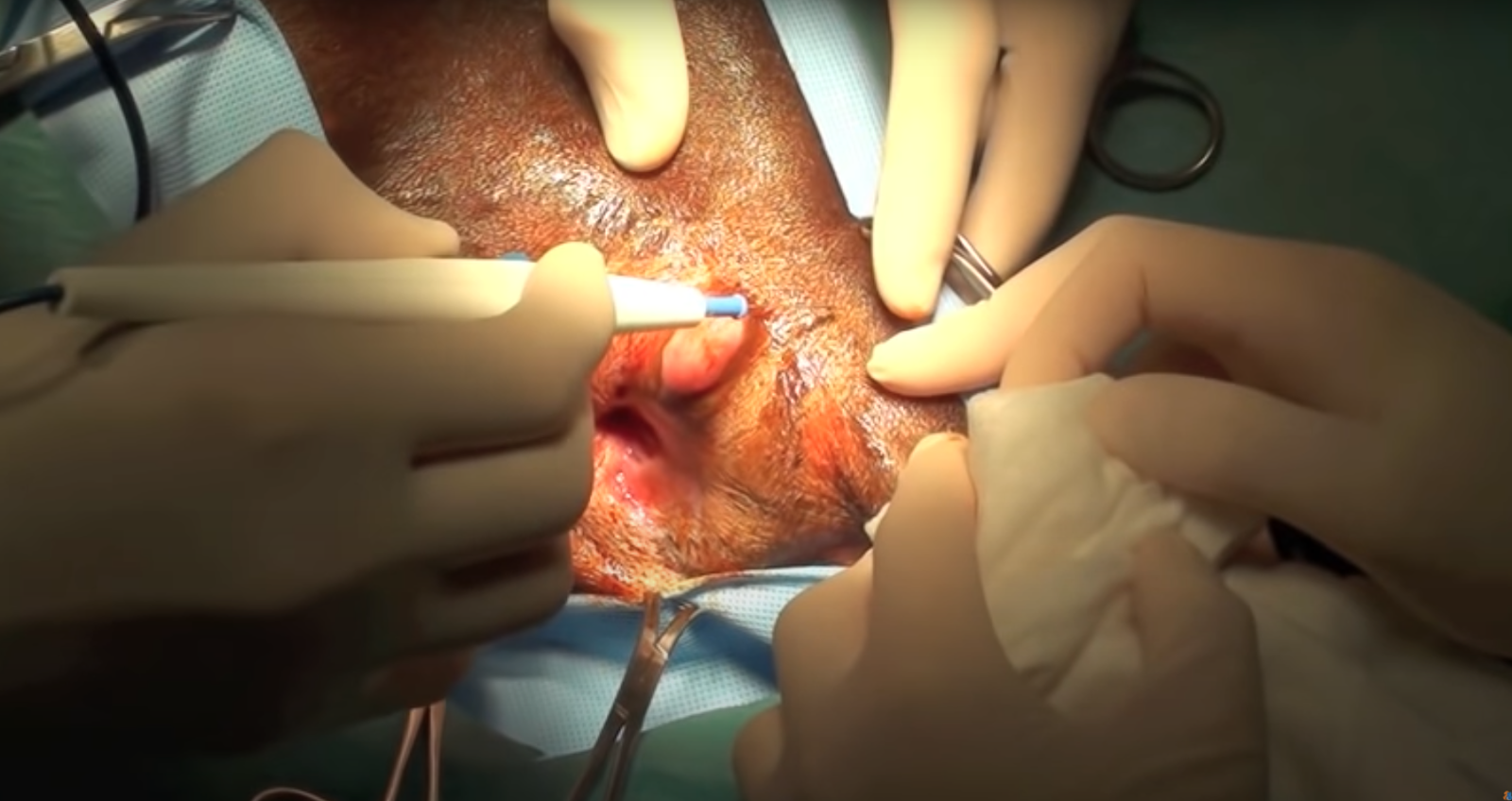
The initial incision is made using a scalpel blade but then as you get through the skin, move to electrocautery.

Use the cautery and cut mode to dissect through the deeper tissues.
The electrocautery is used again for deeper dissection and for haemostasis.

The mast is palpated so that there is a nice layer of loose subcutaneous fat surrounding the mast and to confirm that the margins are clear.

The subcutaneous tissue is sutured around the external anal sphincter to the subcutaneous tissue in the peri-anal region as the first layer of closure.

If you are concerned over the ability to get a tension-free closure, you can use a transposition flap to close the defect, which is harvested using electrocautery in cut mode.
It’s important that the length of the flap is no more than two times the width of the flap or there’ll be issues with vascularity.

Then use electrocautery to elevate the skin from the underlying soft tissues.
You can then use a towel clamp to provide the initial closure for the donor site, which is then closed using subcutaneous sutures.


The rest of the skin is closed using 2/0 PDS intradermal sutures.